
ASM Level Checks for Optimal Seizure Control During Pregnancy
Monthly monitoring of anti-seizure medication (ASM) levels is an important tool for minimizing the possibility of seizures worsening during pregnancy. Pregnancy can increase ASM clearance, and the extent of clearance changes will vary by type of ASM and from patient to patient, so frequent monitoring and adjustment of medication dosages helps maintain optimal seizure control and support the safety and health of both patient and fetus.
This page will provide information and resources to guide clinicians in monitoring ASM levels and making dosage adjustments based on ASM blood levels, also called therapeutic drug monitoring, and seizure frequency.
Topics covered on this page include:
Clinician Role and Communication
If a neurologist is involved in the patient's care, they will typically handle the ordering and monitoring of ASM levels and should be responsible for making necessary dose adjustments to maintain each patient’s target concentration. However, all healthcare providers should be aware of the need for level monitoring and ensure it is being done.
For other clinicians, this means continuously consulting with the neurologist and encouraging patients to follow their advice. It is essential to include ASM-level monitoring as part of the overarching pregnancy plan and engage all members of the care team. Educate your patients about the plan to test and manage their levels and provide them with a schedule of appointments to facilitate proper monitoring and management during this critical period.
Monitoring Anti-Seizure Medication (ASM) Levels During Pregnancy
Monitoring ASM levels is key to a safe pregnancy. To establish a patient's target level for optimal seizure control, the clinician will need to determine the individual’s ideal therapeutic level based on their pre-pregnancy ASM regimen, seizure control, and side-effects. It is most helpful to think of the individualized target level as a range. Assuming seizures are stable, the target range is set at or slightly above the pre-conception level, recognizing that ASM levels will continue to decrease as pregnancy progresses. For instance, for Jacki Smith, the lamotrigine target concentration range may be 2.5-5.0 mcg/ml, but for Alex James, it may be 4.0-7.0 mcg/ml. Doses will need to be adjusted to maintain the individualized target range based on results of the blood levels.
As soon as the patient knows they are pregnant, regular monitoring of ASM levels should begin and then continue approximately every 4 weeks. The frequency of obtaining levels should be adjusted for low levels, new symptoms, seizure worsening, or side effects.
To avoid holding medications to get a trough level, perform blood draws at a convenient time for the patient so that they can get all of their blood draws at approximately the same amount of hours post-dose.
For ASMs that are highly protein-bound, free (unbound) levels are preferable when available (e.g., free phenytoin, free valproic acid, free carbamazepine, free phenobarbital). However, for most ASMs, monitoring of free levels is not required.
Proper monitoring of ASM levels allows for timely adjustments to promote the patient's seizure control and well-being throughout pregnancy.
ASM Blood Levels Throughout Pregnancy Without ASM Dose Adjustments
Data generated from the MONEAD study demonstrates how much ASM concentrations would decrease in each trimester if no dosage adjustments were made. Below are examples from the two most commonly-used ASMs Lamotrigine (Figure 1) and Levetiracetam (Figure 2). Note that there is substantial inter-individual variability, and thus guidance with a patient’s blood level monitoring results is ideal. However, if this is not available, this data can be used as guidance for empiric dose adjustments.
Figure 1
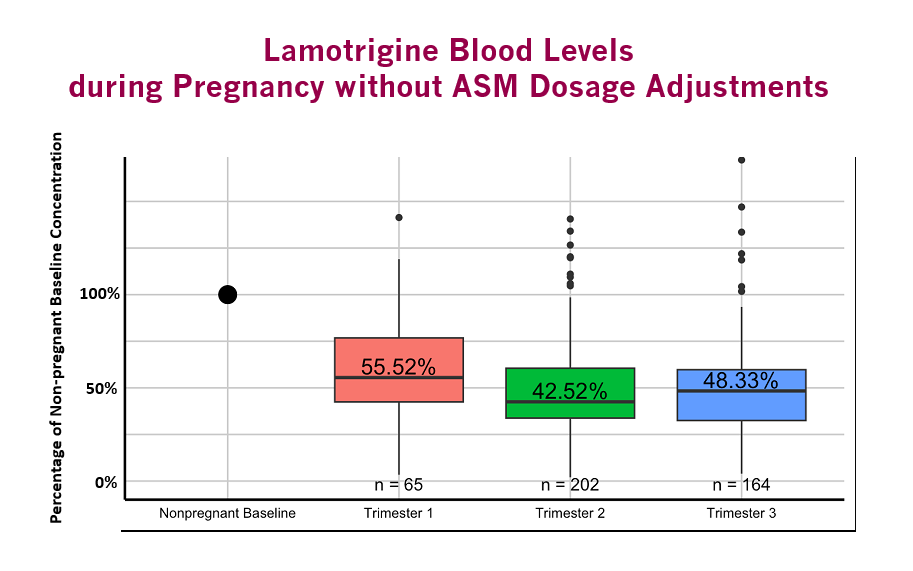
Median ASM dose-normalized concentrations. Box plots represent the 25th and 75th percentiles, and whiskers represent 1.5 times the interquartile range. n= number of blood samples in each trimester. Concentrations were significantly lower in each trimester compared to non-pregnant baseline (p<0.001). Adapted from Pennell PB, Karanam A, Meador KJ, et al. JAMA Neurol. 2022. PMID: 35157004.
Figure 2
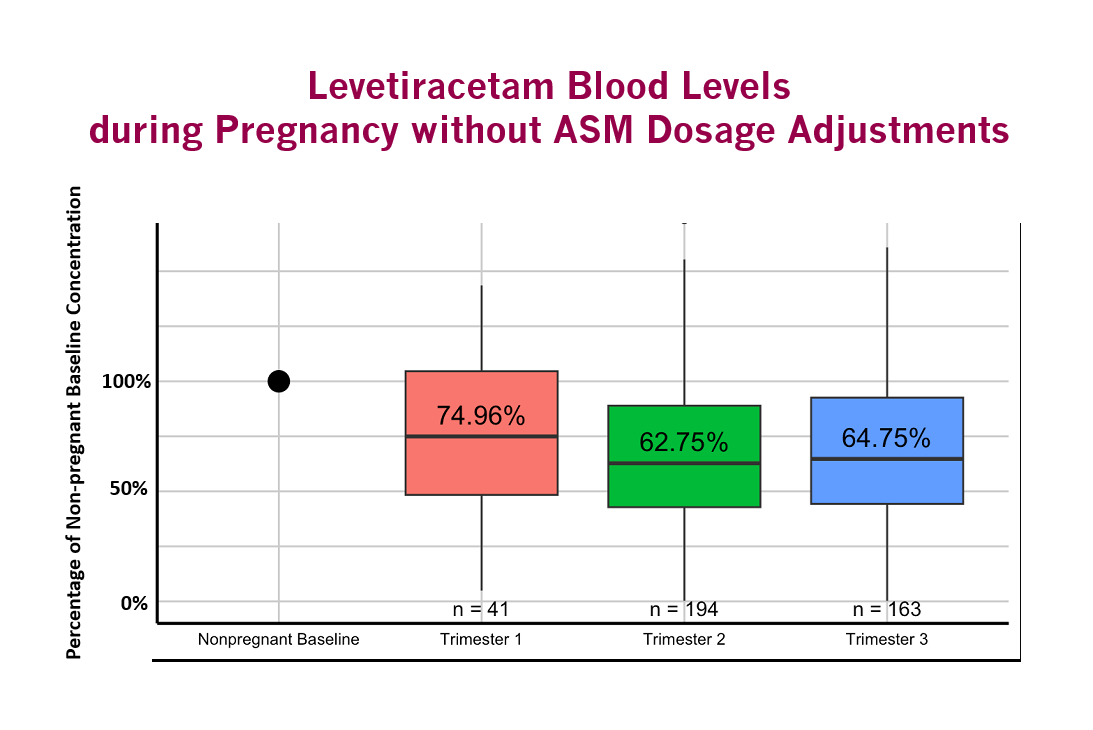
Median ASM dose-normalized concentrations. Box plots represent the 25th and 75th percentiles, and whiskers represent 1.5 times the interquartile range. n= number of blood samples in each trimester. Concentrations were significantly lower in each trimester compared to non-pregnant baseline (p<0.001). Adapted from Pennell PB, Karanam A, Meador KJ, et al. JAMA Neurol. 2022. PMID: 35157004.
When Levels Warrant Anti-Seizure Medication (ASM) Dosage Increases
For most medications, dosage increases are typically recommended under any of the following conditions:
- A fall in ASM blood levels to the lower end or below target range.
- An increase in seizure activity above baseline without a clear trigger (such as missing doses).
In general, do not decrease the dose if the level returns up to 20% above the upper end of the individual’s target range unless the patient is having symptomatic dose-related side effects (e.g., diplopia). ASM levels will keep dropping throughout pregnancy, so even if a level comes back (slightly) higher than the patient’s individualized target range, the dose shouldn’t be lowered unless the patient is complaining of side effects, which may include vertigo, vomiting, blurry/double vision, and ataxia.
In the MONEAD study, the following prescribing patterns by the clinicians were observed for the two most common ASMs, lamotrigine and levetiracetam. During pregnancy, dose increases for lamotrigine were made as 100mg/day increments with changes at 25-35 day intervals, with a mean dose at delivery of 190.5% of conception. Dose increases for levetiracetam were made as 500mg/day increments with changes in 37-47 day intervals, with a mean dose at delivery of 177% of conception. This Pregnancy Planning Tool can be helpful in assisting patients with dosage changes.
Medications that are increased during pregnancy should be tapered postpartum to transition back to an appropriate dosage for the patient. Clinicians will often return to the pre-conception dose plus a small additional amount daily to mitigate the seizure-provoking effects of sleep deprivation. Appropriate dosage adjustments are vital for optimizing seizure management and ASM side effects during this period. The patient should be educated about the signs and symptoms of ASM toxicity and contact their provider if these occur to adjust the tapering dosage schedule.
In MONEAD, the following prescribing patterns in the first 6-weeks postpartum were observed. Lamotrigine was decreased beginning at 2 days postpartum and continued every 4 days until reaching a mean dose that was 116% of the dose at conception. Typical lamotrigine dose decreases were in 100 mg/day increments. Levetiracetam was decreased beginning at 3 days postpartum and continued every 3-5 days until reaching a mean dose that was 136% of the dose at conception. Typical levetiracetam dose decreases were in 500 mg increments.
Managing Anti-Seizure Medication (ASM) Dosage Increases When Blood Levels Aren't Available
When ASM blood levels are unavailable, managing medication dosage for people with epilepsy requires careful consideration and adherence to specific conditions. Keep in mind that certain ASMs are known to undergo significant changes in clearance during pregnancy, including lamotrigine, levetiracetam, and oxcarbazepine.
It is especially important to consider empiric dose increases during pregnancy if any of the following three criteria are met:
- The patient’s seizures include focal to bilateral or generalized tonic-clonic seizures.
- The patient's seizure control was sensitive to changes in ASM levels before pregnancy.
- The patient began pregnancy on the lowest effective ASM dose.
In such instances, clinicians can refer to research reports on how ASM concentrations change during pregnancy and their time course in order to make adjustments. By carefully considering these conditions, you can help your patient make informed decisions to optimize seizure management during their pregnancy.
Guide Your Patients
ASM level checks and potential dosage increases during pregnancy can raise concerns for your patients about medication changes and how they might impact their baby. It is essential to emphasize that therapeutic drug monitoring plays a crucial role in maintaining seizure control during pregnancy and that ASM level checks and adjustments are an important tool to help keep them and their baby healthy.
Frequently, dosage increases are necessary to maintain seizure control as the body clears medicine quicker during pregnancy. Remind your patient that their baby is not exposed to higher medication amounts with these changes since their blood volume is increased and/or the pregnant body metabolizes the medications more quickly; it is a similar concentration as before pregnancy.
Dosage changes are normal during pregnancy, as pregnant patients with most epilepsy often require more frequent medication adjustments than non-pregnant patients. However, continuing medication throughout pregnancy is vital for both the patient’s safety and their baby's well-being. You can also explore our other resources on ASM safety during pregnancy to help guide your patient.
Reviewed by: EPMC Expert Panel, March 2025